The procedure commonly referred to as a Brazilian Butt Lift (BBL) is, at its core, a sophisticated form of autologous fat grafting—a two-part process that redefines body contour by harnessing the patient’s own tissue. This complex operation has evolved significantly from its early, often risky iterations to become a highly refined aesthetic surgery. It is not simply about volume addition to the buttocks; rather, it is about strategic fat harvesting, meticulous purification, and precise placement to achieve a harmonious and natural-looking silhouette. The success of a BBL hinges on the surgeon’s artistic vision, technical skill in handling delicate fat cells, and deep understanding of gluteal anatomy and vascular safety. The transfer of living fat cells involves critical considerations related to graft viability and long-term retention, which differentiate this procedure from the simple injection of synthetic fillers. This discussion will dissect the intricate steps of fat grafting within the BBL context, moving beyond the superficial desire for shape and focusing on the biological and technical realities that govern its outcome.
Fat Grafting is a Two-Part Process that Redefines Body Contour
The initial and crucial phase of the BBL procedure involves the controlled removal of excess fat from specific donor areas, most commonly the flanks, abdomen, lower back, and thighs. This targeted removal, essentially liposuction, is fundamental not only to acquire the necessary graft material but also to sculpt the surrounding areas, which enhances the final projection of the buttocks. The principle of “hourglass illusion” dictates that reducing the circumference of the waist and back creates a more dramatic and aesthetically pleasing contrast with the augmented gluteal region. The technique used during liposuction is paramount; aggressive or high-pressure suction can damage the delicate adipocytes, compromising their survival upon transfer. Therefore, surgeons often employ specialized, low-pressure cannulas and techniques designed to maintain the integrity of the fat cells, treating them as precious, living tissue. The decision of where to harvest the fat is strategic, aiming for areas with a high concentration of viable fat cells that will provide the best long-term volume.
Specialized, Low-Pressure Cannulas and Techniques Designed to Maintain the Integrity of the Fat Cells
Once the fat has been harvested, it must undergo a delicate preparation phase before being reintroduced into the body. The extracted material is a mixture of viable fat cells, oil (from ruptured cells), blood, and excess fluid. To ensure maximum graft survival and minimize the risk of complications, this mixture must be purified. Centrifugation, washing, or filtering are common methods used to separate the healthy, intact fat cells from the unwanted components. The goal is to obtain a concentrated, high-quality graft composed primarily of intact adipocytes. Fat cells that are damaged or mixed with significant quantities of blood or oil are less likely to survive and can contribute to inflammation, fluid accumulation (seroma), or unpredictable absorption over time. This stage is critical because the purity and concentration of the transferred fat directly correlate with the volume retention and the smooth, long-term aesthetic result. A high-quality graft improves the odds of a successful biological “take” in the recipient area.
The Success of a BBL Hinges on the Surgeon’s Artistic Vision
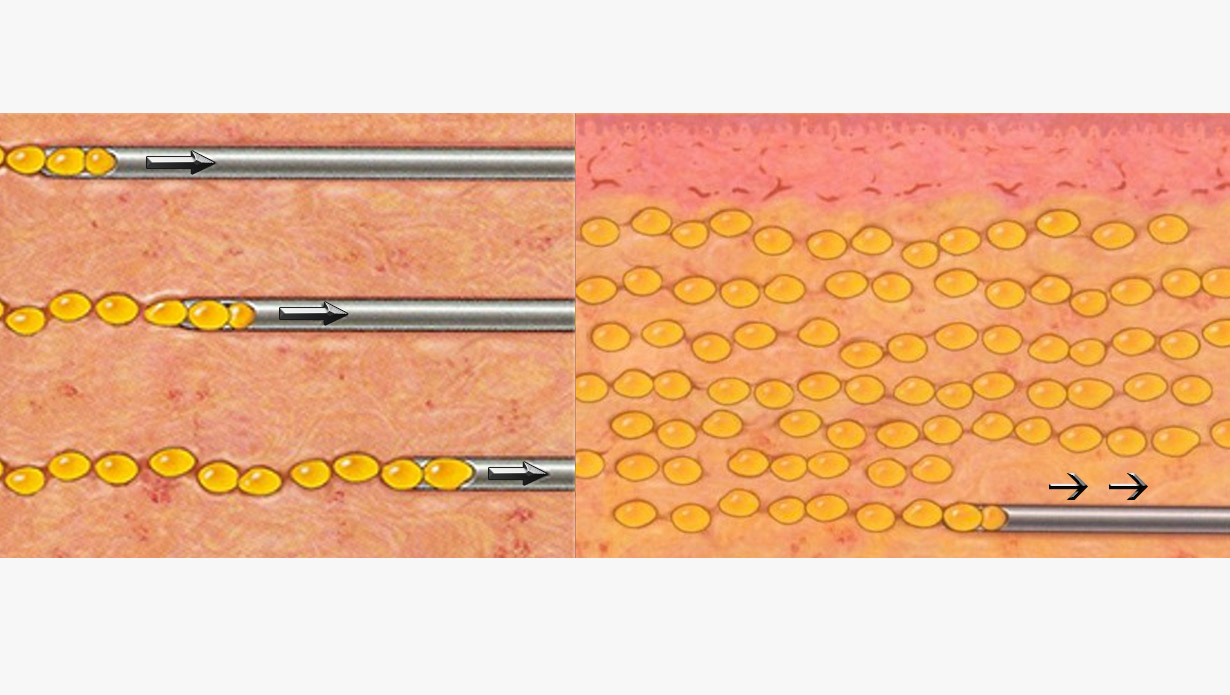
The implantation stage—the actual grafting—moves from the technical realm of harvesting and processing into a surgical art form. The success of a BBL hinges on the surgeon’s artistic vision and technical mastery of injection dynamics. The fat is not simply injected into one mass; it must be dispersed meticulously and evenly across multiple layers and planes within the gluteal region. A skilled surgeon will use fine cannulas to deliver small aliquots of fat throughout the subcutaneous tissue and the intramuscular plane, being acutely aware of the goal to create smooth contours and natural transitions, particularly around the hips and back. This layering technique maximizes the surface area contact between the newly transferred fat cells and the host tissue, which is essential for the cells to establish a new blood supply and survive. Inadequate dispersal or the injection of large, concentrated boluses of fat can lead to central necrosis (fat cell death), lumpiness, and poor long-term retention.
Dispersed Meticulously and Evenly Across Multiple Layers and Planes
A paramount concern in modern BBL surgery is the meticulous avoidance of injecting fat into the deep gluteal muscles and, crucially, beneath the gluteal fascia and into the large, deep blood vessels. Dispersed meticulously and evenly across multiple layers and planes ensures safety. Accidental deep injection carries the devastating risk of injecting fat directly into the gluteal veins, which can lead to a fat embolism—a blockage in the lungs (pulmonary embolism) or heart, often with fatal consequences. Industry standards and surgical guidelines now strictly mandate that fat must be placed superficially, primarily in the subcutaneous plane above the muscle fascia, and only very conservatively into the superficial layers of the muscle itself, if at all. The entire focus has shifted to maximizing safety while achieving the aesthetic goal, recognizing that patient safety is the non-negotiable priority that dictates the injection technique and plane.
The Survival of the Transferred Fat is Not Guaranteed
Patients must be educated that the survival of the transferred fat is not guaranteed; it is a highly variable biological process. Typically, a portion of the grafted fat cells, often ranging from 30% to 50%, will not successfully integrate with the host tissue and will be naturally reabsorbed by the body in the weeks and months following the procedure. This reabsorption occurs because not every transplanted cell manages to establish the necessary blood supply (revascularization) to sustain itself. The initial post-operative volume will therefore gradually decrease until the remaining, viable cells establish permanence. The stability of this remaining volume is achieved approximately six months after surgery. This expected volume loss is a critical consideration for both the surgeon, who must often slightly over-graft to account for the loss, and the patient, who must manage expectations regarding the final, long-term result. Factors like the patient’s post-operative care, compression garment use, and lifestyle choices can influence this final retention rate.
Essential for the Cells to Establish a New Blood Supply and Survive
The mechanism of fat survival, often referred to as the take rate, relies entirely on essential for the cells to establish a new blood supply and survive. In the immediate period following injection, the fat cells that are placed near healthy, oxygenated tissue can survive through simple diffusion of nutrients. However, long-term survival requires neovascularization—the growth of new blood vessels from the recipient site into the grafted fat tissue. This process is actively supported by growth factors present in the transplanted fat and the surrounding tissue. Placing the fat in thin threads, rather than thick clumps, maximizes the ratio of the cell surface area to the volume, thus increasing the chance that all cells are close enough to the host tissue to initiate this life-sustaining process. Poor blood supply due to overly dense packing or placement in scarred tissue is the single biggest factor leading to fat necrosis and subsequent reabsorption or lump formation.
Post-Operative Care is As Crucial As the Surgery Itself
The patient’s compliance with post-operative instructions is not merely a formality; post-operative care is as crucial as the surgery itself in determining the final outcome. Specifically, patients are typically instructed to avoid sitting directly on the buttocks for an extended period, usually two to three weeks, and often longer. Direct, prolonged pressure on the newly grafted fat can compress the delicate new blood vessels attempting to form, thereby depriving the fat cells of oxygen and nutrients and severely compromising the take rate. Surgeons recommend lying on the stomach or using specialized air-filled cushions that redistribute pressure to the back of the thighs. Furthermore, the mandatory use of compression garments on the donor areas helps reduce swelling and promotes skin retraction, enhancing the contouring achieved through liposuction, though the garment for the buttock area must be carefully chosen to avoid excessive, damaging pressure on the grafts themselves.
The Patient’s Overall Health and Lifestyle Can Influence the Outcome
The biological reality of the BBL procedure means that the patient’s overall health and lifestyle can influence the outcome in profound ways. Smoking, for instance, significantly impairs blood flow and oxygen delivery throughout the body, directly hindering the necessary neovascularization process and substantially reducing the fat graft survival rate. Patients who smoke are often advised to cease nicotine use for a period both before and after the surgery. Similarly, significant fluctuations in weight following the procedure can alter the augmented shape. The transferred fat cells retain their biological characteristics, meaning they can still swell and shrink with weight gain and loss, respectively. Maintaining a stable, healthy weight post-surgery is essential for preserving the newly achieved contour and maximizing the longevity of the results, as dramatic weight changes will inevitably affect the volume and shape of the grafted area.
Aesthetic Harmony Across the Entire Torso is the True Goal
While the focus is often placed exclusively on the volume and projection of the gluteal area, the true measure of a successful BBL is often its subtlety. Aesthetic harmony across the entire torso is the true goal of the operation. This involves the thoughtful contouring of the waist, lower back, and flanks to transition smoothly into the augmented buttocks. A surgeon who understands this concept will not merely add volume but will sculpt the periphery to create a visually continuous, balanced, and proportionate figure that complements the patient’s individual frame. It is the careful balance between fat removal (liposuction) and fat addition (grafting) that achieves the desired transformation, moving the body from a square or rectangular shape to one that flows organically, avoiding the telltale signs of isolated, unnatural augmentation. The final result should appear as a naturally full and shapely contour, not a singular, isolated feature.
Not Every Patient is an Ideal Candidate for Fat Grafting
A critical distinction must be made: not every patient is an ideal candidate for fat grafting or a BBL. The procedure is inherently dependent on the patient having sufficient, high-quality fat in suitable donor areas. Individuals who are very lean (low body mass index, or BMI) may not possess enough harvestable fat to achieve the desired volume enhancement safely. Attempting to harvest marginal amounts of fat can lead to poor donor site results and an insufficient graft volume, often resulting in disappointing or unstable buttock augmentation. For these patients, alternative methods or a staged approach involving initial weight gain may be necessary. A thorough pre-operative consultation is essential to establish realistic expectations based on the patient’s unique anatomy, fat distribution, and overall health profile, ensuring that the goals of the procedure align with the biological and technical possibilities.